5th Metatarsal Fracture Support
The fifth metatarsal is one of the long bones that sits on the outside of the foot, and it connects to the midfoot area, through the cuboid at one end, and at the other end, it connects to the little toe.
These fractures are almost always caused by an inversion injury. An inversion injury is the movement you make when you roll your ankle. In fact, there are times when a person will think they have an ankle injury when they actually have a fifth metatarsal fracture. They can also be caused by repetitive microtraumas which are called stress fractures.
Orthotics Plus provides acute support to people in Melbourne who have sustained a 5th metatarsal or lower limb fracture.
Types of 5th Metatarsal Fractures
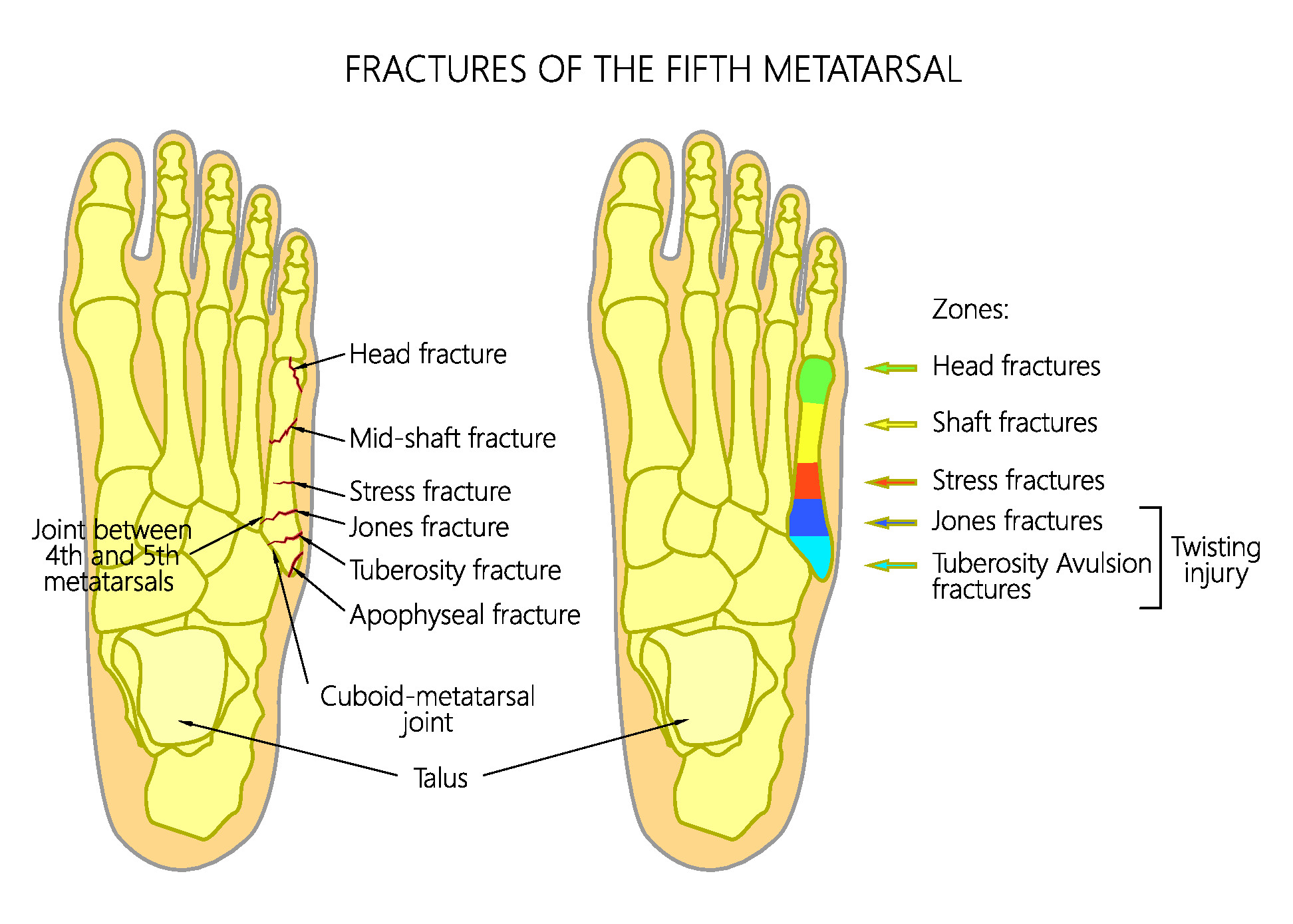
5th metatarsal fractures can be divided into different categories, depending on the location of the fracture and the mechanism of injury.
- Avulsion fracture – often known as a ‘base of the 5th fracture’, the mechanism of injury is the ankle inverts forcefully and the tension of the peroneal tendon pulls off a small segment of bone in the area which has good blood supply. These fractures usually heal quite well.
- A Jones fracture – a type of fracture that affects a specific area of the metatarsal, where there is poor blood supply. The fracture line is further down the metatarsal than a ‘base of the 5th’ fracture. They can be caused by trauma, or repetitive loading. These fractures often require surgery or orthopaedic management.
- Mid-shaft or ‘Dancers fractures’ – these are less common and can be due to trauma or twisting movements. As the name suggests they occur in the middle of the metatarsal bone.
NB: Stress fractures. These fractures are caused by repetitive loading which exceeds the capacity and healing ability of the bone. Common in distance runners or people returning to loading after time off. People with poor biomechanics, poor footwear choice and with high arched foot posture are more susceptible to stress fractures. The pain usually occurs on the outside of the foot and the stress fracture location is in the proximal third of the metatarsal.
When there is a 5th metatarsal fracture it is common to see an ankle sprain affecting the anterior talofibular ligament or a peroneal (which attaches to the base of the 5th metatarsal) injury, as seen in the video.

Treatment Process for 5th Metatarsal Fractures
If you have sustained an injury, you can contact emergency or your GP, both of which can refer for an x-ray.
If the incident is acute, there is a high chance that you will be given a back slab as a temporary measure. You will then be referred for your next stage of recovery. This may be a referral to Orthotics Plus for an appointment and fitting of a moon boot. This can be the same day as the injury.
Before or after this time, you will attend x-ray appointments, which is the standard procedure over CT/MRI scans. Your healthcare team will review the x-rays, confirm the type of fracture and act accordingly. If referred to Orthotics Plus we suggest bringing in your x-rays for review, as we have on occasion noticed things the hospitals have missed.
Treatment will often involve pain medication, elevation and compression stockings to control the swelling. The Moon Boot will be critical equipment to support the patient’s rehabilitation as it will provide immobilisation, callouses and healing.
Your weight-bearing status will depend on your injury and your pain levels.
While a cast is a possible treatment option, there are very few occasions we actually use one. This is because they are inconvenient in terms of not being waterproof or able to weight bear. CAM walkers or ‘Moon Boots’ are much more comfortable and functional.

Risks of 5th Metatarsal Fractures
Non-Union – A non-union is a fracture that doesn’t heal and remains fractured unless there is surgical intervention.
Atrophy – there is going to be a degree in muscle loss during rehabilitation. This is because of increased immobility and decreased usage of the limb. The calf is the most affected area.
Deep Vein Thrombosis – There’s always a risk of DVT for legs when they are non-weight bearing for some time, though, it’s not very common for 5th metatarsal fractures.
If a patient’s pain or swelling increases in or around their fracture site, this can be a sign of DVT and the patient should report this to their health team asap.
Stress Fracture Management- Post Acute Phase
Once you have recovered from your stress fracture, it is highly suggested to liaise with an Orthotist to assess your biomechanics, footwear and foot posture. It is likely you will benefit from foot orthotics in the short to mid-term to unload the lateral aspect of your foot and prevent the recurrence of the stress fracture.
If your stress fracture injury was due to running, we suggest being pain-free for 2 weeks before beginning a running program.
It is also suggested to work with a physio or EP to develop a running program to allow your body to adapt to the load you are putting through it as these injuries can recur.

Need Fracture Support? Contact Orthotics Plus
As a provider of acute care for over a decade, Orthotics Plus is a professional and appropriate to consider for your fracture rehabilitation.
- We offer same-day bookings
- We work with multiple hospitals, GPs and radiographers around Melbourne
- We are university qualified
- We are highly experienced in fracture management
We look forward to hearing from you. Please view our clinic locations to get started.

FAQ
Yes to both.
It is very important that we read this information.
This is because the diagnosis of this type of fracture can be difficult to articulate. For example, we have seen radiography reports that state the injury is a Jones fracture when in fact, it is the base of the metatarsal, and vice versa.
It is important to have us (who specialise in the foot/ankle) check the x-ray and educate our patients on the correct terminology for their case.
Yes.
At Orthotics Plus, we believe that high arching (cavus foot postures) are at higher risk of certain types of fractures. Higher arched feet load the outside of the foot more and are often more rigid in their structure. This can mean higher loads in the areas prone to stress fracture.